

Post-traumatic arthritis
Lateral osteophytes have to be ignored when placing head in correct position, the head should the be tilted into valgus without risk of notching. The osteophyte at the medial head neck junction has to be removed before the head guide can be placed in the planned position on a straight neck – the guide should sit stably. Beware hips with adduction contracture – the hip may well be externally rotated on the 2D XR so check – the hip may be less valgus when internally rotated. Guide settings 25/J/-4.
Mild dysplastic hip, with normal head neck relationship
The head is downsized slightly, positioned so that the medial head neck junction is covered, then oriented into slight valgus. Medial necks like this can be tricky – the two medial jaws of the head guide need to be positioned far apart to ensure a stable base. Even after a stable construct is delivered, the stylus checks are essential to ensure that the 2d plan is an accurate representation – the real neck-shaft axis may be less valgus than on XR. Guide settings 30/G/-2.
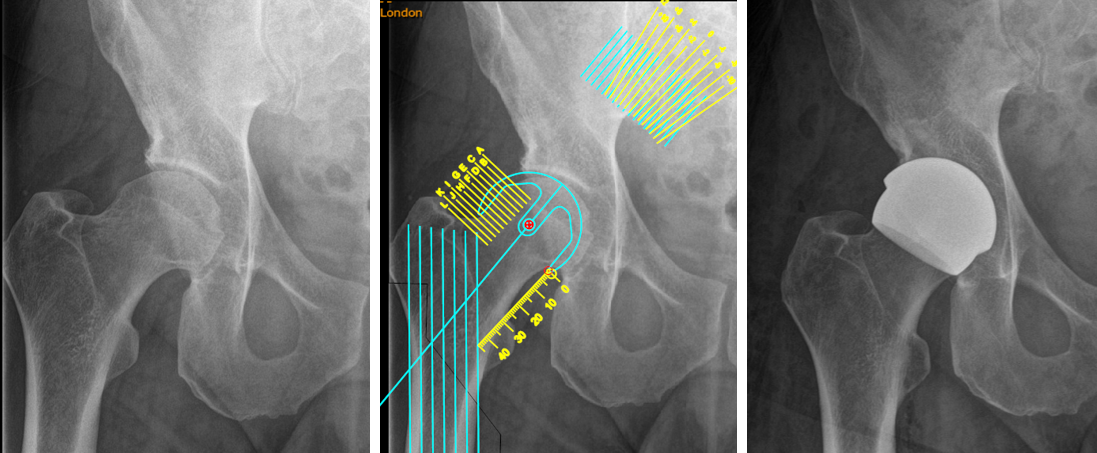
Male cam hip
Horizontal offset will be reduced on the femoral side so don’t deepen the socket. The head is lateralised and put into valgus. In this case the head-neck junction isn’t osteophytic, but is curved, so maximise the planned length between the two medial jaws of the head guide. Intra-operatively, check that the scale is right on the head, and on the medial neck – it may be over- or under- estimating the size. Guide settings 25/I/4.

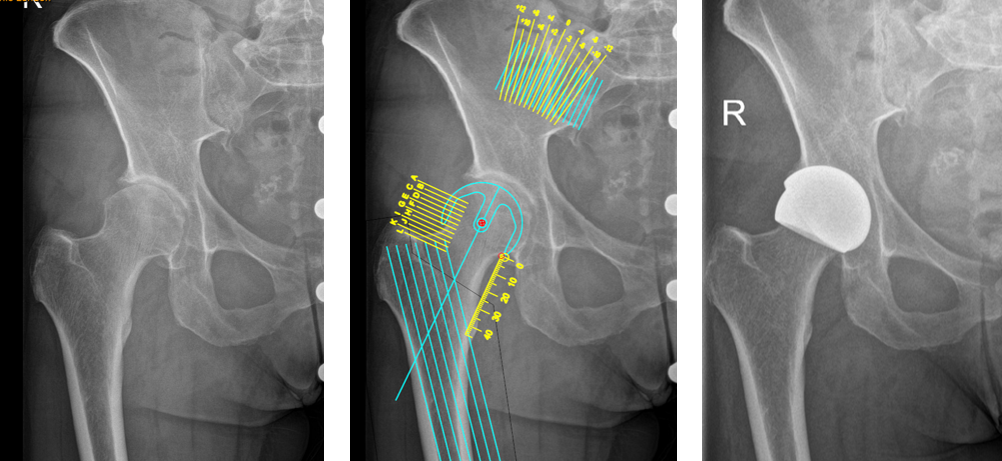
Male dysplasia and an anterior cam
Horizontal offset will be reduced so don’t deepen the acetabulum. The head has to be positioned at the medial head neck junction, allowing the osteopaenic medial bone to be resected. The component is then tipped into as much valgus as is safe. The head guide medially should take advantage of the length of the neck. Intra-operatively check that both medial jaws of the head guide are on bone medially. If either is held off, the head will be dragged medially risking a notch. Guide settings 28/H/-2.